山寨币评测:SOL 会上涨吗? LUNC 是多少美元?
- 来自 比特派钱包官网
- 04-26, 2024
加密的最新发展营造了一种完全不确定的氛围。 减半发生后,市场出现了波动,但这种波动并没有持续多久。 在此过程中备受关注...




比特派采用业内领先的安全技术,用户的私钥仅存储在自己的设备上,确保资产的绝对控制权和安全性,免受黑客入侵、平台跑路等风险。

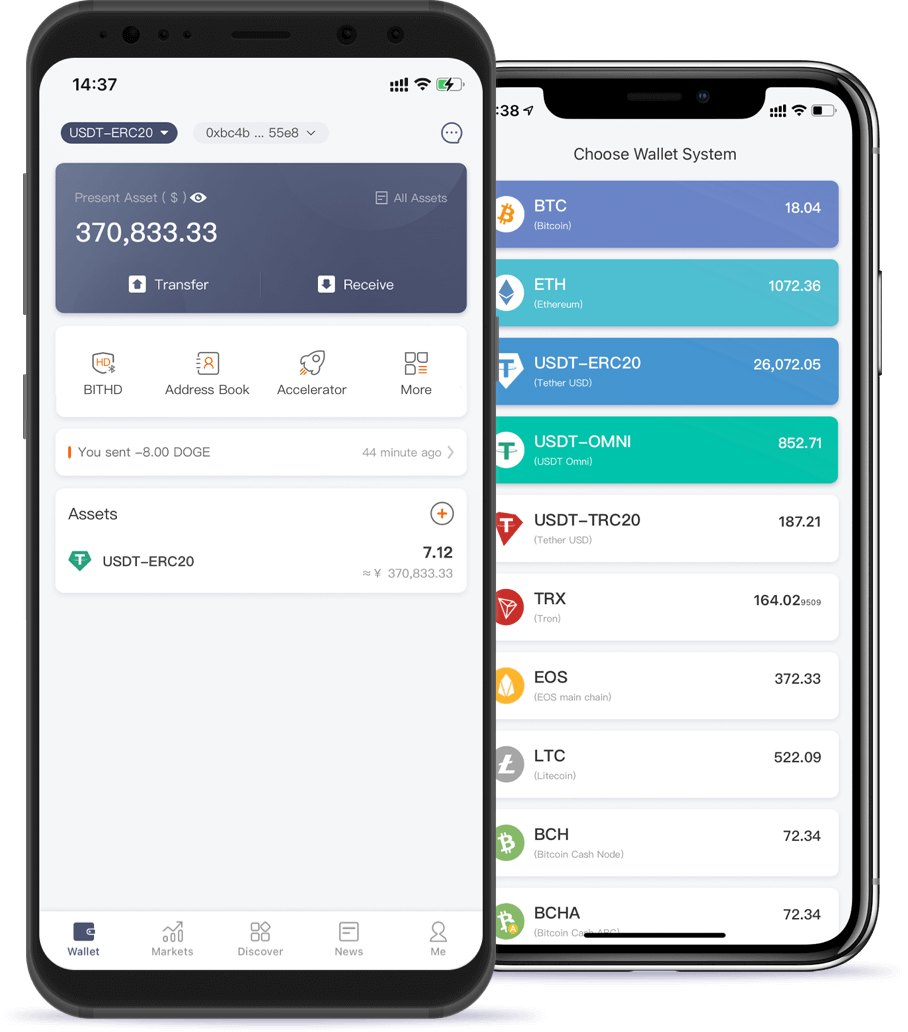
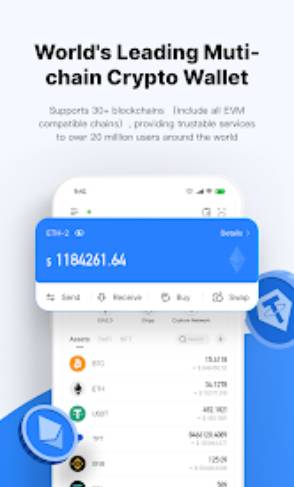
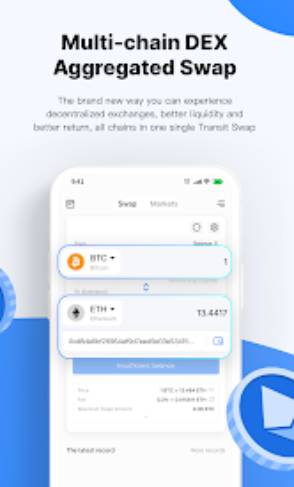
比特派支持BTC、ETH、ERC20等主流公链资产,并对币圈热门项目持续导入,让用户能够在一个钱包内便捷管理不同链上的数字资产。

比特派与ledger等知名硬件钱包完美兼容,用户可将比特派钱包与硬件钱包无缝连接使用,实现资产冷热钱包的无缝切换,最大程度保障资金安全。


轻松访问 BTC、ETH、BNB、TRX、DOT、MATIC、LTC、BCH、ATOM、OP、FIL、ARB、EOS、KSM、XTZ、CKB

比特派钱包搭配硬件钱包,离线签名更安全




比特派钱包(bitpie)是业内领先的通用加密货币钱包,支持超过200种主流数字货币,包括比特币、以太坊、EOS等。Bitpie钱包安卓/iOS正版App拥有顺畅的操作体验,强大的资产管理功能,并提供专业的行情分析和教育内容。立即前往比特派官网,免费下载Bitpie最新版钱包App,体验安全可靠的加密货币管理!
比特派钱包是我在加密世界中的得力助手!它的多链支持让我能够轻松管理我的各种数字资产,而且DeFi功能也让我能够参与各种有趣的项目。强烈推荐!
作为一个对数字货币投资的新手,我一直觉得钱包的安全性和易用性很重要。比特派满足了我的这两个需求,操作非常简单直观,私钥绝对安全,让我可以放心地管理和使用自己的数字资产。
比特派钱包对于钱包的安全性重视程度很高,采用了很多先进的技术保护用户资金安全,同时也很注重用户体验,界面设计漂亮实用。作为一个老用户,我对比特派钱包的整体表现很满意。
之前我的数字货币资产分散在好几个不同的钱包里,管理起来很不方便。现在有了比特派这款多链钱包,可以将所有资产都集中在这一个钱包里,无缝切换,大大简化了操作,让我重新拥有了对资产的掌控感。
比特派钱包给了我一个便捷的方式来管理我的加密资产。我喜欢它的安全性和多链支持,但有时候在进行交易时会遇到一些费用较高的情况。
比特派钱包的DeFi集成非常方便,但我希望它能够增加更多的教育资源,帮助用户更好地了解和使用DeFi产品和服务。
我从不写评论,但认为这是值得的,已经使用加密货币几个月,并且总是难以购买加密货币并快速获得它这是一个很大的帮助购买了 .5 eth 并且能够在 5 分钟内使用它








比特派钱包(bitpie)是业内领先的通用加密货币钱包,支持超过200种主流数字货币,包括比特币、以太坊、EOS等。Bitpie钱包安卓/iOS正版App拥有顺畅的操作体验,强大的资产管理功能,并提供专业的行情分析和教育内容。立即前往比特派官网,免费下载Bitpie最新版钱包App,体验安全可靠的加密货币管理!

加密的最新发展营造了一种完全不确定的氛围。 减半发生后,市场出现了波动,但这种波动并没有持续多久。 在此过程中备受关注...

随着 2024 年牛市即将到来,精明的投资者正在密切关注有望带来丰厚回报的加密货币。 领先者是 BlockDAG (BDAG),其先进的方法和强大...

总长DR随着 Rebel Satoshi ($RBLZ) 通过 Monarchs 加密货币 ICO 第 4 轮的进展,投资者表达了看涨情绪。顶级加密货币分析师预测 THOR…...

5-6 年前,大多数投资者不会想到 SEC 会批准现货比特币 ETF。 然而,截至2024年1月,比特币已经成为在美国交易所交易的ETF。 净流入...

毕马威 (KPMG) 在日耳曼国家进行的一项最新调查显示,所有 2400 名参与者的投资组合中超过四分之一是加密货币。 Bison 是德国最大的...